If you have been in scientific or analytical circles at all, you have heard the admonition, “Correlation is does not mean causation” or something similar. That is, for two events, or outcomes or results that we simply label as A and B, there may be a correlation, but it does not mean that A causes B or that B causes A. The following example makes this very clear.
In the early half of the 20th century, polio was a devasting disease that took the life of many young people or left them permanently disabled. The cause was unknown and there was considerable medical and scientific effort to understand the cause and thereafter a search for a cure.
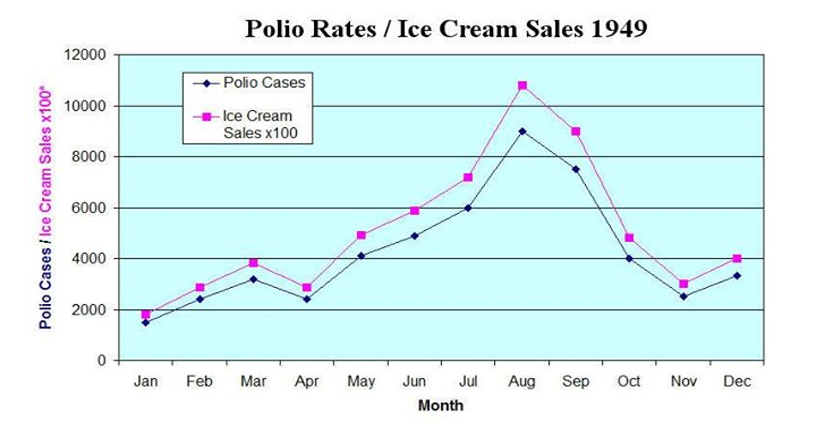
One interesting relationship is depicted in the figure below, which shows the monthly number of new cases of polio and the consumption of ice cream for the year 1949. When plotted on this common scale, the two curves move in lock step, exhibiting a very high correlation. In fact, children were instructed to refrain from ice cream in order to reduce their chances of contracting the debilitating and sometimes deadly disease (https://theglyptodon.wordpress.com/2012/08/21/polio-caused-by-ice-cream/).
What we now know is depicted in the following schema or causal diagram. Polio is a
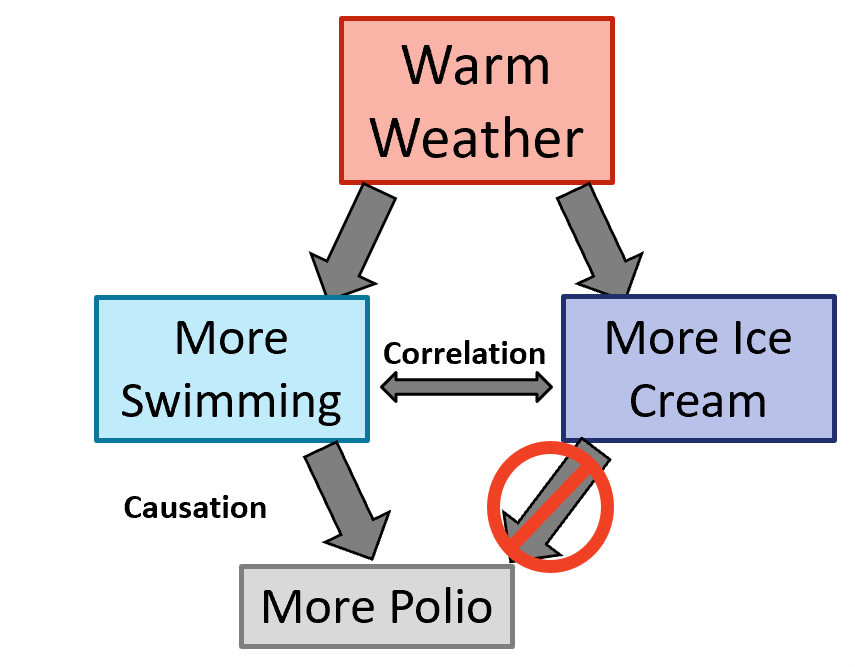
virus that is readily transmitted via contaminated water. Warm weather provides the opportunity for more swimming in public pools and other places that facilitated the spread of the disease. Warm weather also produces a greater interest in the cool and tasty delights of ice cream. Thus, both disease incidence and ice cream consumption move up and down as the temperature rises and falls, but A (ice cream consumption) does not cause the outcome B (polio).
OK, this example seems trite today, but was not so in the middle of the last century. Of course, we have learned not to be fooled by such incidental correlations … or have we?
In discussing a modern article on associations, please keep in mind two things:
- The term “correlation” is often used synonymously with “association” or “linked to;”
- When describing the relationship between A and B, if it is stated that A is associated with B, then it is equally fair to describe the relationship as B is associated with A. That door swings both ways.
Now, on to a modern scientific article.
The Lancet, Psychiatry published an article entitled “Association of disrupted circadian rhythmicity with mood disorders, subjective wellbeing, and cognitive function: a cross-sectional study of 91 105 participants from the UK Biobank.”( https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(18)30139-1/fulltext) I chose this article for the simple reason that last year, I was listening to my local public radio station and an interviewer from the BBC World Service was talking to (I believe) Daniel Smith (Institute of Health and Well-Being, University of Glasgow) who is one of the co-authors. Because of what I perceived as a disconnect between the interviewer and Dr. Smith, as well as the description of the research findings, I thought I should investigate this a little further.
I won’t get into all the details of the research (as I noted in my Introductory blog … I am not and cannot be an expert in all fields of science, but I can play the role of expert in inference), but suffice to say, the study was as advertised in the title – associations in circadian rhythm and mental health. It involved a very large group of people whose medical records are in the UK BioBank (https://www.ukbiobank.ac.uk/about-biobank-uk/). Note that circadian rhythm in this study was measured by an accelerometer (https://axivity.com/product/ax3), a device that measures motion, and the authors categorized patients into low and high activity (using a measure of relative amplitude from the accelerometer).
The key findings of the study and the concise summary provided by the authors states:
“Interpretation: Circadian disruption is reliably associated with various adverse mental health and wellbeing outcomes, including major depressive disorder and bipolar disorder. Lower relative amplitude might be linked to increased susceptibility to mood disorders.”
In simple language, let A = circadian disruption (quantified by activity/motion) and B = adverse mental health and wellbeing (they examined a long list of mental health conditions and performance measures). So, A is associated with B. However, the use of the word “outcomes” with B gives a subtle implication that A comes first and then B is the “outcome,” which connotes a causal link.
Are you sure?
The Interpretation could have just as reasonably been written to say B is associated with A; that is, adverse mental health and wellbeing is associated with circadian disruption (outcomes?). Does one precede the other? Does sleep disturbance (one example of a circadian disruption) lead to mental health issues? Or do mental health issues lead to sleep disturbances? Or neither, since there may be no causal link. Perhaps, like the polio examples, there is confounding variable that produces both observations independently of each other. Perhaps there is some biochemical disturbance in the brain (like warm weather) that manifests as disturbances in circadian rhythm (like ice cream) AND mental health issues (like polio).
Similarly, stating “Lower relative amplitude [calculated from the accelerometer] might be linked to increased susceptibility to mood disorders.” gives a very different feel (at least in my mind) than to state, “Increased susceptibility to mood disorders might be linked to lower relative amplitude [activity level of the patient].”
The phrase “might be,” which shows up in a lot of association studies, usually catches my attention as well. I would much prefer a more quantitative evaluation that, for example, would state, “There is a 76% probability that <insert whatever relationship is relevant>.” A statement such as “There is a 39% probability that <insert whatever relationship is relevant>” can also be described in English language terms as “might be associated” but is VERY different than the “might be associated” statement when the probability is 76%. Your “might be” threshold and my “might be” threshold can be very different, and without more explicit quantification, a conclusion that states “might be” is not very informative.
To the authors credit (at least a little bit), of the 8 pages devoted to this article, there are a couple sentences where the authors address causality. They state, “… the current findings cannot speak to the issue of causal associations between circadian disruption and poorer mental health and wellbeing outcomes. … Our goal was to look for evidence of cross-sectional associations rather than to infer causality. Future work … will be useful in elucidating the nature and direction of causality.”
Since we are most interested in causal effects in scientific research (i.e. understanding cause and effect), I sometimes question such research that does not seek to estimate, establish or infer causality. It is interesting that the authors state the “nature and direction of causality.” I would add to their list elucidating IF there is any causal relationship at all. Thereafter, IF there is a causal relationship, elucidating the direction – whether A causes B or B causes A – is worthwhile.
If association studies are meant to develop surrogate markers of disease that are easier and cheaper to measure or provide an “early warning system” for the onset of disease, then that is valuable. The authors devote only two sentences (the last two) and a vague allusion to this notion when they state, “Relative amplitude is relatively cheaply and easily measured and might be useful for identifying people at greater risk of major depressive disorder or bipolar disorder, or subgroups of patients who might benefit from therapies aimed at improving circadian rhythmicity.” However, there is an implication of cause and effect. The first part of the sentence suggests relative amplitude is predictive of developing future mental health disorders (i.e. risk), and the second half of the sentence states that improving circadian rhythmicity could help subgroups of patients with mental disorders (i.e. treating rhythmicity and improving it will improve a patient’s mental health).
What is noteworthy of this research, in my estimation, is that we might be able to put a wrist-watch accelerometer or other actigraphy device on a patient and have some objective measures to complement subjective evaluations of a patient’s mental health status by a trained health care professional. Ultimately, such a device might even be able to accurately classify who is suffering from depression or bipolar disorder better than a trained psychiatrist, just as machine learning and AI are learning to read medical images from patients to diagnose diabetic retinopathy or malignant cancers. Thus, the accelerometer watch would represent a cheaper, more objective diagnostic that does not require an expensive and time-consuming office visit. Unfortunately, the authors seem to nudge us to the boundaries of cause and effect more than the potential use of circadian rhythmicity as a surrogate measure or diagnostic for mental disorders.
It is that nudge that caught the attention of the BBC interviewer and filled her line of questioning of Dr. Smith. She kept using (as I recall the radio interview … BTW, I could not recover a transcript of the interview from the BBC, but if anyone can …) the notion that poor sleep habits cause mental health issues, and Dr. Smith rightly corrected her using the word “associated.” But they were like ships crossing in the night. There is more to say about analytical thinking and this article, but further comments will be relegated to a future blog.
If you want to see an example of Data Scientists and the (over?)use of association studies that link human behaviors (as measured by digital devices, including our smart phones) with health outcomes or disease states, visit www.evidation.com and look under the Research tab. I cannot keep up with all their publications, but at least my rough impression is that they have a little more reasonable understanding of the use of such associations as diagnostic or surrogate measures that could take the place of expensive or difficult to measure clinical outcomes or disease states.
So, whenever I read about an association between A and B, I like to …
- First, reverse A and B in the statements or conclusions and see how that sounds.
- Second, pay close attention to language that conveys or subtly suggests causal effects (e.g. “outcomes” or “risk” in this example).
- Third, assess whether the research is pursuing causal relationships or doing what is rightly reasonable – looking for reliable surrogate measures of our health status (i.e.correlation).
I have heard a Partner of a large business consulting company and self-proclaimed Data Scientist say, “We do not need causation anymore. Correlation is enough with big data.” If you ever hear such nonsense from someone, just tell them the polio and ice cream story … and then run from whatever they are selling.
I hope this blog is correlated with your interests and has helped you develop a healthy skepticism when reading about associations.

Great example! I plan to use this with my STA 301 classes at Miami University next semester.
LikeLike
Lisa,
Yeah! I am glad you like it and can use it with students. That’s one of my goals is to provide material that people can use for educating others (students, scientists or other professionals) about analytics thinking.
Keep the cards and letters coming. I hope you find other materials helpful.
AND SPREAD THE WORD!
Thanks.
LikeLike